The leaflet is detailed below, or you can download the 'Predictive Genetic testing for Lynch Syndrome' leaflet in PDF
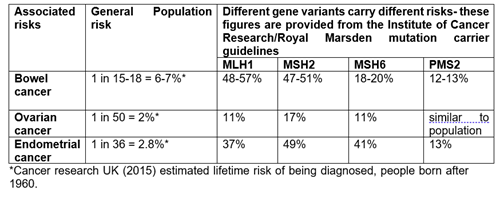
Cancer is common in the general population in the UK, with 1 in 2* people being diagnosed with a cancer during their lifetime. Most cancers are due to chance and/or environmental factors. For example, we know that the chance of developing cancer increases as we get older, and that lifestyle factors such as smoking, drinking alcohol and being overweight increase the chance of developing many cancers. Some cancers occur due to inherited genetic factors. We are more suspicious of there being an inherited cause for the cancers in a family if the same or related cancers occur across multiple generations, are diagnosed at younger than expected ages, with more people developing cancer than we would expect by chance.
*Cancer research UK (2015) estimated lifetime risk of being diagnosed, people born after 1960
What are genes and chromosomes?
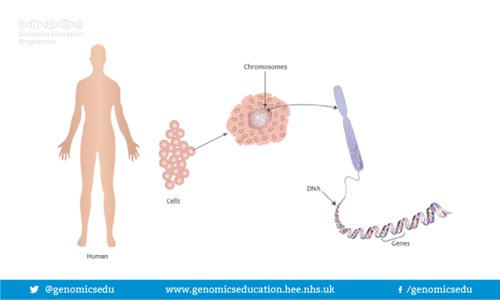
Humans are made up of trillions of cells. At the centre of almost all of your cells is a ball-shaped structure called the nucleus, inside of which are 46 thread-like structures called chromosomes. Chromosomes are long strands of DNA (DeoxyriboNucleic Acid). It is estimated that if a strand of DNA was stretched out, it would be around two meters long, even though the average cell is smaller than a pinhead.
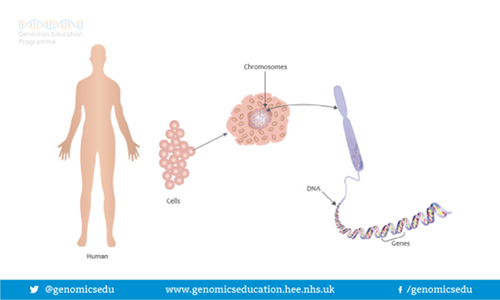
Image source: https://www.genomicseducation.hee.nhs.uk/image-library/
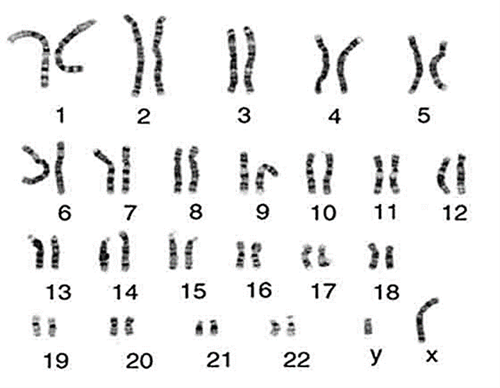
Image Source: https://cpmc.coriell.org
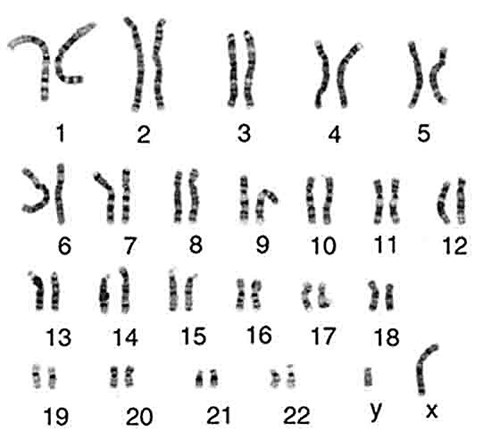
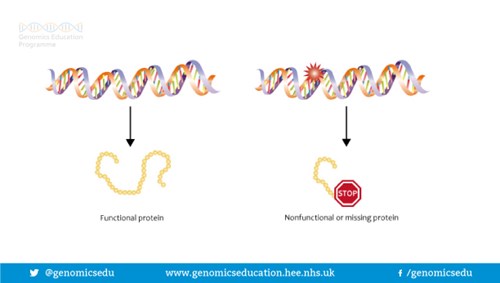
We have 23 pairs of chromosomes and one of each pair is inherited from each parent. Chromosomes contain an estimated 20-30,000 pairs of genes. Genes are often called the blueprint for life because they tell each of your cells what to do and when to do it. For example, some genes determine how tall you will be; some what colour your hair will be; some genes are responsible for maintenance in our bodies and some for our development. Genes do this by making proteins. In fact, a gene may act by being a ‘recipe’ or a code for making a certain protein. In order for a gene to do the job it is supposed to do, the ‘recipe’ or code needs to be written correctly. If the ‘recipe’ is wrong, the protein is either not made, or is made incorrectly so cannot do the job it is supposed to do. This is sometimes called a gene variant, a spelling mistake or a mutation.
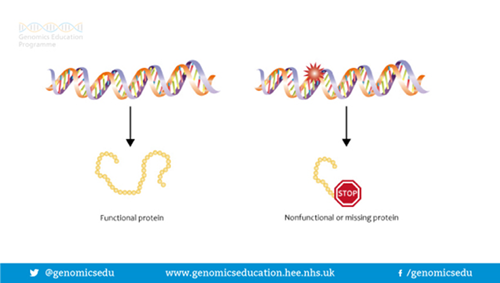
Image source: https://www.genomicseducation.hee.nhs.uk/image-library/
What is Lynch syndrome?
Lynch syndrome is a hereditary condition that causes people to have an increased chance of developing certain types of cancer. Lynch syndrome used to be known as Hereditary Non-Polyposis Colorectal Cancer (HNPCC).
There are currently 4 mismatch repair genes that we know of that act like a quality control system; MLH1, MSH2, MSH6 and PMS2. They help protect us from developing cancer by detecting and correcting errors that can occur in DNA when cells copy themselves (DNA replication errors). Having a pathogenic variant in one of these genes means that the quality control system is less effective and the person has Lynch syndrome, and so is more likely to develop certain types of cancer. Having Lynch syndrome does not mean a person will definitely go on to develop cancer.
Having Lynch syndrome causes a high chance of developing bowel cancer. People with Lynch syndrome who were assigned female at birth also have a high chance of endometrial (womb) cancer and often a high chance of ovarian cancer, depending on the particular gene in which the pathogenic variant is found. Additional screening and/or risk-reducing measures may be advised depending on individual risks. There may also be a slightly increased chance of developing other cancers including kidney (renal) cancer and pancreatic cancer but not enough to warrant routine screening unless there is a family history. It is important to have a low threshold for seeking medical help for any concerning or persistent symptoms.
What are the main cancer risks associated with having Lynch syndrome?
What can be done to help manage these increased risks?
|
Management option
|
MLH1
|
MSH2
|
MSH6
|
PMS2
|
|
Colonoscopy screening
|
Every 2 years aged 25-75
Review at 75
|
Every 2 years aged 25-75
Review at 75
|
Every 2 years aged 35-75
Review at 75
|
Every 2 years aged 35-75
Review at 75
|
|
Gastric screening
|
H Pylori one off screening from 25
|
H Pylori one off screening from 25
|
H Pylori one off screening from 25
|
H Pylori one off screening from 25
|
|
Aspirin chemoprevention
|
Discuss with GP the pros and cons of taking aspirin, further details below
|
Discuss with GP the pros and cons of taking aspirin, further details below
|
Discuss with GP the pros and cons of taking aspirin, further details below
|
Discuss with GP the pros and cons of taking aspirin, further details below
|
|
Risk-reducing gynaecological surgery
|
Surgery to remove the womb, ovaries and fallopian tubes (hysterectomy and bilateral salpingo-oophorectomy)
No earlier than 35-40 and once childbearing complete
HRT should be offered until 51 in women who have not had ER +ve breast cancer
Everyone with a cervix should attend for their regular cervical smears
|
Surgery to remove the womb, ovaries and fallopian tubes (hysterectomy and bilateral salpingo-oophorectomy)
No earlier than 35-40 and once childbearing complete
HRT should be offered until 51 in women who have not had ER +ve breast cancer
Everyone with a cervix should attend for their regular cervical smears
|
Surgery to remove the womb, ovaries and fallopian tubes (hysterectomy and bilateral salpingo-oophorectomy)
No earlier than 35-40 and once childbearing complete
HRT should be offered until 51 in women who have not had ER +ve breast cancer
Everyone with a cervix should attend for their regular cervical smears
|
Surgery to remove the womb (hysterectomy)
No earlier than 45 and once childbearing complete
Everyone with a cervix should attend for their regular cervical smears
|
| |
|
|
|
|
|
|
|
|
|
What does a colonoscopy involve?
A colonoscopy is an internal examination of the large bowel. The purpose of a colonoscopy is to look for bowel cancer and polyps.
Polyps are quite common in the general population, but they are very common in people with Lynch syndrome. Most polyps are harmless and will not cause any trouble. However, some polyps do have the potential to turn cancerous if left to grow over time, as illustrated:
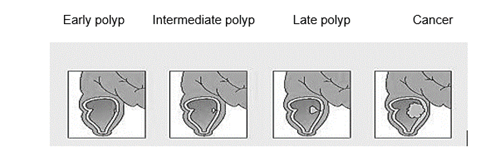
Image source: NHS National Genetics and Genomics Education Centre
By removing any polyps during a colonoscopy, this reduces the chance of them turning cancerous.
What does gastric screening involve?
People with Lynch syndrome should also be tested for the presence of a bacterium called Helicobacter pylori (H.pylori) and this can be done through your GP. H.pylori can live in the gut and can lead to chronic gastritis which in turn could lead to an increased risk of stomach cancer for people with Lynch syndrome. H.pylori can be detected by a breath test, blood test or stool sample and if found, eradicated with a course of antibiotics.
Why should I discuss aspirin use with my GP?
Aspirin taken daily for 2 years or more could reduce the risk of colorectal (bowel) cancer in people with Lynch syndrome, says National Institute for Clinical Excellence, NICE guidance 151. Aspirin is not licensed for this purpose so if it is prescribed for cancer risk reduction this is called an ‘off-label’ use of aspirin.
The best dose of aspirin is not yet clear, but the UK Cancer Genetics Group recommend those between 25 and 65 years consider taking 150mg if 70kg or under and 300mg for people who weigh more than 70kg. These recommendations are likely to be updated over the coming years as more evidence becomes available.
PLEASE REMEMBER; Aspirin is a drug that can have serious side effects. It should never be taken without first being reviewed by your GP to make sure there is no reason you should not take it. We are not recommending consideration of aspirin usage to anyone without Lynch syndrome.
Can I have screening for ovarian and endometrial cancer rather than surgery?
Screening for ovarian cancer and endometrial cancer is not proven to be effective in detecting these cancers at an early enough stage in order for them to be treated effectively. Therefore, it is advised that people with Lynch syndrome who have a womb (and/or ovaries) consider risk-reducing gynaecological surgery as detailed above.
What else can I do to help protect my health?
We encourage people to not smoke, to maintain a healthy BMI, to limit their consumption of red and processed meat, and to exercise regularly. Doing these things can all help to reduce the chance of developing many types of cancer.
How is Lynch syndrome passed down (inherited) through families?
Lynch syndrome is inherited in an autosomal dominant inheritance pattern. We have two copies of each of the mismatch repair genes and if one copy has a variant then this means the person has less protection against developing certain types of cancer and they have Lynch syndrome. Each time someone with Lynch syndrome has a child, there is a 50% chance of passing on the working copy of the gene and a 50% chance of instead passing on the gene variant causing Lynch syndrome. Someone with Lynch syndrome has usually inherited this from one of their parents.
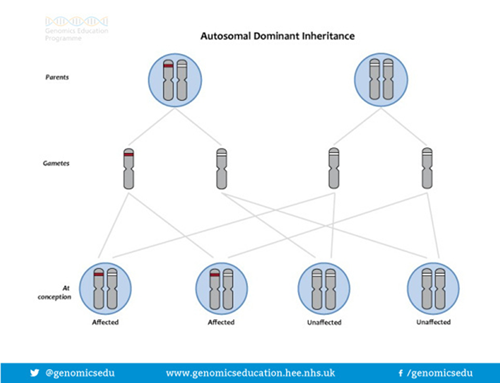
Image source: https://www.genomicseducation.hee.nhs.uk/image-library/
What is predictive testing?
Predictive testing is offered to family members who may have inherited a specific gene variant that has been identified in the family. Predictive testing is usually offered over a series of appointments to allow the opportunity to consider options and choices with time for reflection in between. How many appointments a person requires varies considerably from person to person and is agreed on an individual basis with your genetic counsellor team. The overall aim of the predictive testing process is to help prepare you for your results whatever they are.
NB: Test results are reported based on current knowledge. Very occasionally, new information in the future may mean that our understanding of the significance of a specific gene variant may change.
What are the issues to think about when deciding whether or not to have a gene test?
A predictive genetic test tells us whether or not you have inherited the specific gene variant known to cause Lynch syndrome in your family. It can be difficult to make a decision about whether or not to have a predictive test and there are reasons for and against it. Within one family, relatives often have different views. You should try to make your own decision, without feeling pressured from relatives or other influences. You will have plenty of opportunity to talk through the issues surrounding the test with the genetic counsellor or doctor.
How do you think you would cope if the test were to show that you have Lynch syndrome?
For some people, knowing that they have inherited the gene variant causing Lynch syndrome is preferable to living with the uncertainty of not knowing. Having a genetic test enables them to make decisions about the future and about screening and measures to reduce their risk. Other people may prefer not to have the test because they may feel very anxious if the test shows that they have Lynch syndrome.
How do you think you would cope if the test were to show that you have not inherited the familial gene variant?
Perhaps surprisingly, it can often take people some time to get used to the knowledge that they do not have the gene variant. This can be particularly difficult when other relatives have a different result.
People who have not inherited the gene variant have the same chance of developing cancer as other people in the general population.
What are the possible implications for children?
Having a genetic test may be important to other people, such as your children. It will help them to understand their own risk and if necessary make choices about screening and risk reducing options.
It can be very difficult knowing that you could have passed on the gene variant to your children. This can be hard to deal with even if you know that you had no control over which genes you passed on. Predictive testing for Lynch syndrome is offered in adulthood as there is not thought to be any increased risk of cancers in childhood.
If you were to have the test, would you want to tell anyone the test results?
It is important to think about who you would want to know about your test as it is very personal information. Many people who attend our clinic find that it helps to confide in a partner, trusted friend or relative.
Would having the test affect your ability to get life or medical insurance?
At present, if you have already obtained your insurance, having the test should not affect your current policies. However, it is not possible to know whether it will affect your ability to get or to change insurance policies in the future.
Would having the test affect your employment?
If the test shows you have Lynch syndrome it would be your decision whether or not to inform your present employers. Some employers might ask about this if you apply for a new job.
It is important that each family member makes the decision that is best for them. We will support you whether you decide to have the test or whether you decide against having the test. It is your decision!
What happens if I choose to go ahead and have a test?
After you have had the opportunity to discuss the positives and negatives of predictive testing, if you wish to have the test you will be asked to read and sign a consent form and a small blood sample will then be taken.
Once the blood is taken, the scientists in the genetic laboratory would test the sample to find out whether or not you have inherited the gene variant known in your family.
Test results are usually available 4-6 weeks after having your blood taken and you can choose to have your results over the phone or in a clinic appointment.
IF, FOR SOME REASON YOU, HAVE NOT RECIEVED YOUR RESULTS WITHIN 4-6 WEEKS AS EXPECTED PLEASE CALL THE LIVERPOOL CENTRE FOR GENOMIC MEDICINE ON 0151 802 5008. Please remember to have your G number and W number handy for this call so we can quickly and correctly identify you.
What happens if I choose not to go ahead with having a test?
We may still recommend screening to you as explained earlier in this leaflet.
You can change your mind and decide not to have the test at any time before the result is given.
Other factors to consider
Insurance and Genetics
For some types of insurance it is necessary to provide medical information, including genetic information, to the insurers in order for them to set up your policy and work out your premiums. The types of policy that require a medical history or genetic test are likely to be, life cover, critical illness insurance and income protection insurance.
We would suggest that if yourself or family members are considering taking out new insurance policies in the future that consideration be given to the possible affect genetic test results could have on the ability to gain insurance or the premiums charged. Genetic Test results do not affect insurance policies already in place.
The Association of British Insurers (ABI) has a Code of Practice ‘The Concordat and Moratorium on Genetic and Insurance’.
- Insurance companies cannot ask for the Predictive Genetic Test results of individuals or family members (unless for Huntington Disease over £500,000). A Predictive Genetic Test is where an individual has a family member with a genetic condition, but who personally has no symptoms, signs or abnormal medical tests consistent with the condition at time of testing.
- If a family member has been diagnosed with a genetic condition based on a Diagnostic Genetic Test then you or family members will need to mention this when asked to provide your family’s medical history. In many cases Diagnostic Genetic Testing is used to confirm a diagnosis when a particular condition is suspected because of symptoms, signs or abnormal non-genetic tests including unusual findings on a routine blood test or other test.
Sources of Further Information on insurance and genetics:
The Association of British Insurers Genetics Frequently Asked Questions https://www.abi.org.uk/products-and-issues/topics-and-issues/genetics/genetics-faqs/
Genetic Alliance UK (Charity) Genetics & Insurance http://www.geneticalliance.org.uk/information/living-with-a-genetic-condition/insurance-and-genetic-conditions/
Family planning
Everyone who has an inherited genetic condition can choose from a variety of options to ensure they do not pass it on. It is a highly personal decision and there is certainly no expectation that couples have to do anything to prevent passing on Lynch syndrome, but for couples who wish to consider this, some of the choices can include:
- Preimplantation genetic testing (PGT-M)
Pre-implantation genetic testing (PGT-M) is a special type of in vitro fertilisation (IVF) which is available to couples who have an increased chance of having a child with a specific genetic condition. The aim is to avoid passing on the genetic condition to the child.
More information can be obtained at https://www.guysandstthomas.nhs.uk/our-services/pgd/about-us/welcome.aspx
- Adoption
- Sperm or egg donation: dependent on who carries the gene variant
Our experience is that very few people who have Lynch syndrome choose any of the above options.
We hope you find this leaflet useful and please do not hesitate to discuss any of the issues identified in this leaflet with the genetics practitioner that is looking after you:
Liverpool Centre for Genomic Medicine Liverpool Women’s Hospital NHS Foundation Trust Crown Street Liverpool
L8 7SS Telephone: 0151 802 5001 or 5008
Email: lwft.clingen@nhs.net






 Pic3
Pic3




 How is the ATM gene alteration inherited?
How is the ATM gene alteration inherited?